Trastuzumab is a monoclonal antibody that has been engineered to attack and block the human epidermal growth factor receptor 2 (HER2), a protein that contributes to cancer cell growth. It is used most frequently to treat HER2-positive breast cancer and HER2-positive gastric cancer. As a targeted agent, trastuzumab has greatly enhanced treatment outcomes for patients with tumors that overexpress HER2.
Mechanism of Action
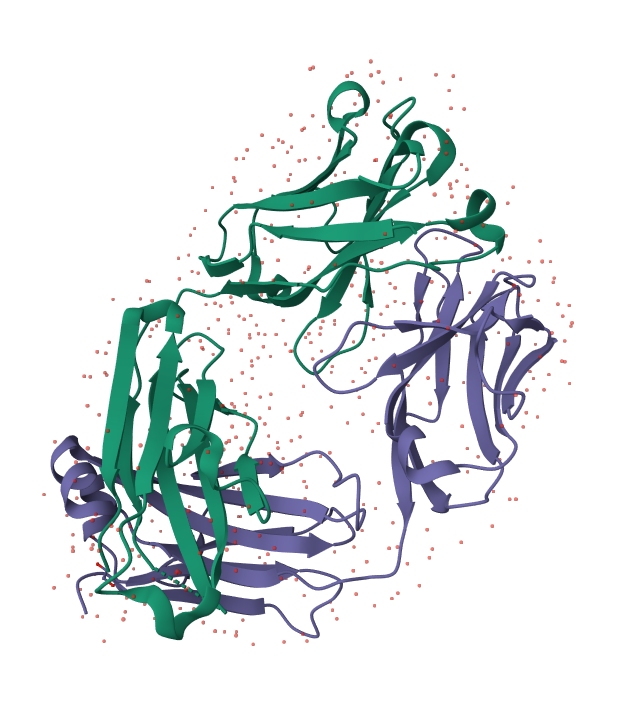
Trastuzumab is a humanized IgG1 monoclonal antibody that selectively binds to the extracellular domain (subdomain IV) of the HER2 receptor. HER2 is overexpressed in nearly 20–25% of breast cancers and correlates with high-grade tumor growth and poor prognosis.
- Inhibition of HER2 signaling: Binding of trastuzumab prevents receptor dimerization and activation, disrupting downstream signaling pathways such as the MAPK and PI3K/AKT pathways, which are essential for cell proliferation and survival.
- Antibody-dependent cellular cytotoxicity (ADCC): Trastuzumab engages immune cells to bind to and kill HER2-overexpressing cells.
- Prevention of HER2 extracellular domain shedding, which prevents formation of a truncated, constitutively active receptor.
Pharmacokinetics
Absorption and Distribution: After intravenous dosing, trastuzumab is distributed in the plasma space. A subcutaneous presentation, usually co-administered with hyaluronidase to promote absorption and dispersion, also exists for some indications, providing a less invasive method of administration. The average apparent volume of distribution is around 44 mL/kg. It is unknown whether trastuzumab crosses the blood-brain barrier significantly.

Metabolism and Elimination: Intracellular metabolism to peptides and amino acids is believed for trastuzumab after it binds to HER2. Elimination is mainly through the reticuloendothelial system by IgG clearance mechanisms. Renal elimination is negligible. The elimination half-life of trastuzumab has been approximated as 28 days, but this may be affected by tumor burden and other patient factors such as weight and levels of serum albumin.
Approved Indications
HER2-Positive Breast Cancer
Adjuvant Treatment: For HER2-overexpressing node-positive or node-negative (estrogen receptor/progesterone receptor [ER/PR]-negative or with one high-risk feature) early breast cancer in adult patients. It may be used as a component of a regimen with doxorubicin, cyclophosphamide, and either paclitaxel or docetaxel; with docetaxel and carboplatin; or as a single agent after anthracycline-based multi-modality chemotherapy. Adjuvant treatment duration is generally up to 52 weeks.
Metastatic Treatment: As a treatment for adult patients with HER2-overexpressing metastatic breast cancer. It may be used together with paclitaxel as a first-line therapy or as a single agent in patients who have received one or more chemotherapy treatments for metastatic disease. In postmenopausal women, it may also be used together with an aromatase inhibitor.

Efficacy
- Enhances disease-free survival (DFS) and overall survival (OS) in HER2-positive breast cancer that is in its early stages.
- Improves progression-free survival (PFS) and response rates in metastatic situations.
- Increases chemotherapy’s effectiveness when combined because of synergistic processes.
Administration and Usage
Trastuzumab is given intravenously or subcutaneously, depending on the product. Therapy initially can be initiated with a loading dose followed by maintenance dosing every 1–3 weeks, depending on the clinical practice and product form. Subcutaneous forms facilitate easier administration, particularly in the outpatient environment.
Side Effects
- Cardiotoxicity: A concern in particular when administered together with anthracyclines. Regular monitoring of left ventricular ejection fraction (LVEF) is necessary.
- Infusion reactions: Frequently experienced in the first few times they are administered, but generally manageable.
- Pulmonary toxicity: Uncommon but severe.
- Mild side effects: Fever, nausea, fatigue, diarrhea, and rash.
Last Modified: